When I look back upon this day in future, I am hopeful that I will recognize it as a major positive turning point in George’s Parkinson’s journey. After patiently waiting to be included in this trial for several months, it finally began!
The official title of the study is “Quantifying Motor Behaviors of Individuals with Parkinson’s Disease.” George’s neurologist partnered with University of Tennessee Department of Engineering to develop a technique to employ sensors to collect data about his motion quality (e.g., acceleration, speed). Sensors were attached to his wrists, his ankles, and around his waist. The researcher observed him using a walker to walk up and down a hallway, to turn, and repeat the process several times.
Thanks to his increased activity lately which included more walks, George handled the first part of the study with relative ease. He usually needs the assistance of a walker to ensure stable movement, and the doctor provided one of the “old style” walkers that only has wheels on the front. It was harder to maneuver than the walker he uses at home; however, he did it. (I think he was highly motivated to “perform well!”) There was only one time during the hour-long test where he needed to stop, sit, and rest. I was very proud of him for his good attitude.
Part 2 of the study will involve a return to the doctor’s office to have sensors applied for use at home. Then, over a seven-day period, he will wear sensors and perform various at-home tasks. All of that data will also be collected for future study.
An important goal of this study is to learn if the neurologist and patient can accurately predict when “off” or “freezing” times will occur during a typical day. This will be invaluable for finding ways to switch those “off periods” to more fluid movements. Even though this study is still in its early stages, I can see great benefits, not only to George but also to other people with Parkinson’s.
If you are like me, you are a technology fan. Participating in this study made me UT Engineering’s “Number 1 Fan!”
Have you ever thought you needed a vacation from your vacation? Well, I have! As usual, it has been a flurry of activity around the Butler abode, but I had the pleasure of having a change of pace recently.
I went to the beach, my happiest of happy places. It was a joy to be there with my daughter’s family and the grandboys. Splashing, playing in the sand, walking along the beach, and partaking of wonderful Gulf seafood, all brought back fond memories of my childhood. It was indeed a treat. For my person with Parkinson’s, not so much.
Prior to the trip, I obviously had to ensure that round the clock caregivers, medications, and household tasks were all in order. George experienced some anxiety because it always seems that he worries when I travel. Travelling was a common occurrence for me in my career, but I don’t think he ever got used to it, and his fears of flying and potential terrorist activity of course increased after September 11, 2001. I flew to Pensacola Florida, so I had to check in with him each time my plane landed; first in Atlanta, then in Pensacola. I rented a car in Pensacola to drive to Orange Beach, so I had to check in again once I arrived at the condo. (It was a beautiful drive along the coast!) Those check-in calls were a small price to pay for alleviating George’s anxiety!
I actually think that it was good for George for me to be gone for a few days, as his independent, old self returned briefly. He handled some business matters, and if I had been home, he would have looked to me to do those things.
My travel down and back was uneventful, which is the way I like it. Only “adventure” I had on the trip was when my daughter and I rented bicycles for a brief ride. All was fine until some other people approached us on the asphalt path. The steering on the bike was wonky, I became nervous over the folks heading toward me, and I didn’t want to collide with them. Instead, I tumbled onto my right knee on the ground. It was mostly my pride that was injured, but there was a plethora of red blood streaming from the abrasions! That was a small price to pay for proving that I could still ride a bike, despite the fall, so I like to think of my cuts as a “red badge of courage!”
On Friday evening after I returned to Knoxville, after George had done well all week with no falls, and good humor, he became tangled up in a tray table that was next to his recliner. He just couldn’t negotiate the pivot that he needs to do to turn and get in the chair safely. Sometimes when he’s fallen in the past, he’s been able to roll over and pick himself up by grabbing onto his walker or a sturdy piece of furniture. However, that night he was fatigued and didn’t have the energy. Thankfully, I was able to call our son who came to help.
Falling does not have to be inevitable for anyone–doing balance exercises, regular walking with proper posture, yoga, Tai Chi, etc., can help everyone as they age. I intend to continue yoga classes before I ride a two-wheel bike again, and George and I will focus on helping his balance. Now I’m rested from my vacation and my knee has healed!
One of the most important things for People with Parkinson’s and their caregivers to remember, is that it is essential to keep moving. Perpetual motion is our watchword!
This week, it was my privilege to volunteer to deliver food for our church’s food pantry, FISH. This was a good thing, as I’ve been somewhat down lately. As we all know, caregiving for a person with Parkinson’s is not for the faint of heart. Daily demands add up, and some days I do not feel up to the task. Lack of sleep makes each day challenging.
Then a day comes along like last Thursday. Even on our worst days, George and I know we have plenty (sometimes too much) to eat. That is not so for those families that FISH serves. These families rely on more than 100 FISH volunteers for survival. I left our house that morning, in worry and fear about George’s condition; but our fridge and pantry were full. Upon my return, I realized that I had delivered a few loaves and canned goods to alleviate hunger for a little while; but, I gained so much more than I gave those families. I forgot about my worries and fears and was grateful for all the blessings that God has given us.
Yesterday’s Gospel lesson recounted the time when Jesus fed the multitudes. Miraculously, five barley loaves and two fish fed more than 5000 people. Afterward, Jesus walked on the sea which terrified the disciples. Jesus said to them: “It is I; do not be afraid.”
Parkinson’s Disease creates fear and trembling, both literally and figurately. The person with Parkinson’s, as well as his or her caregiver, struggles with maintaining an optimistic outlook. And, I am reminded of the immortal words of Franklin D. Roosevelt who, in encouraging Americans to pull out of the Great Depression, said: “The only thing we have to fear is fear itself.”
Our society today has many hungry people. How are they to be fed? they require spiritual as well as physical food. Material things can feed the body, but only love can feed the spirit.
My FISH experience helped me to set aside fear and anxiety for a time. Focusing on the needs of others has a way of doing that. Go and love someone today!
The National Parkinson’s Foundation website states:
With medical marijuana now legalized in 29 states and Washington, D.C., it is obvious that there is strong interest in its therapeutic properties. Researchers are testing marijuana, which is also called cannabis, as a treatment for many illnesses and diseases, including neurological conditions, with Parkinson’s disease (PD) high on the list. But despite several clinical studies, it has not been demonstrated that cannabis can directly benefit people with PD.
Indications
While there is limited evidence that has been gathered evaluating cannabinoid medicine and medical cannabis use as treatment for Parkinson’s Disease, there is a wealth of information on the effects of these options on symptoms often experienced by patients with Parkinson’s Disease, such as pain and sleep disturbance. According to a post on the Parkinson’s Disease Foundation website by Blair Ford, M.D., “Descriptions of Parkinson’s Disease do not generally include the mention of pain. And yet, when carefully questioned, more than half of all people with Parkinson’s disease say that they have experienced painful symptoms and various forms of physical discomfort.” There is mounting evidence that cannabis may be useful for some patients in managing chronic pain. Additionally, evidence for relief from symptoms experienced by patients with Parkinson’s Disease, such as depression and anxiety, has been discovered with the use of cannabinoid therapy. Cannabis use may also provide relief to patients experiencing nausea and vomiting, potential side effects of certain standard PD medications. Pain, depression, and anxiety can be arguably more debilitating for people with Parkinson’s than the movement disorder itself. Therefore, why hasn’t more research been done?
No large, placebo-controlled, randomized, double-blinded clinical trials have been conducted on the effect of whole-plant cannabis on patients with Parkinson’s Disease, meaning that there is no evidence that a cause-effect relationship exists showing that cannabis use improves symptoms or slows progression for patients with Parkinson’s Disease.
When the evidence on cannabis in relation to a certain disorder is limited, we can turn to patient stories for anecdotal evidence that medical marijuana may provide relief for some patients, especially those with symptoms uncontrolled by standard therapies. A recent blog post, “The goal of medicine is to balance evidence with stories” highlights the important point which is its title. Given the favorable safety profile of medical cannabis and potential for low-risk experimentation for most patients, patient stories help in guiding healthcare professionals to which symptoms/disorders may be alleviated by the use or study of cannabinoid medicine.
According to David Esparza, a patient who has lived with Parkinson’s Disease for over 13 years and has experienced negative side effects from standard therapy, “[Cannabis] helps me with my attitude, it helps me with my shaking, it helps me deal with my new life… I don’t know how I look to other people… but I know what I feel like [when using cannabis]… I feel good.” He shares his story here.
According to a study published in Journal of Neurology, Neurosurgery and Psychiatry in 2013, the cannabinoid THC (the psychoactive cannabinoid) also may prove useful in the treatment of Parkinson’s Disease by (1) assisting in the prevention of damage caused by free radicals and (2) activating PPARγ, a receptor whose stimulation leads to the formation of new mitochondria (the part of cells that produces energy).
Additionally, there is mounting evidence that cannabinoids have the potential to work as neuroprotective agents (i.e. those that protect destruction of neurons) through processes such as improvement of function of mitochondria and the activation of cellular debris clearance. Increased research will help us to explore and harness any potential neuroprotective effects of cannabinoids. Please click here for more information on the potential for cannabinoid medicine use in the treatment of neurodegenerative diseases.
Summary
It is clear that more research is needed to determine what, if any, benefit may be derived from cannabis. Given today’s political climate (namely an Attorney General of the United States who appears to profit from incarcerating drug offenders) and the power of pharmaceutical companies to block anything that is not one of their products. However, the use of cannabis for medical use is now legal in Tennessee. Those of us who suffer from Parkinson’s, or are Parkinson’s caregivers, must lobby our legislators (at both the state and federal level) to ensure that we receive the best information, the best therapies, and the best drugs to treat this monstrous disease
One of the first things that elementary school music classes teach Kindergartners and First Graders is how to keep a steady beat. This is fundamental to all rhythmic learning, so it is stressed early. Learning how to clap their hands, pat their knees, or stamp their feet are good physical ways to imprint this skill.
As a musician, I find that 60 beats per minute is a favorite, comfortable tempo. I think that may be because 60 beats per minute is also a good resting heart rate. A good heart rhythm (steady beat) and heart rate are indicators of good health. The heart is a vital physical organ. But, the term “heart” can also refer to one’s soul or spirit. Spiritual health is just as important as physical health, so care should be taken with both.
Recently, George started looking for a stethoscope that he purchased shortly after his heart surgery. Neither one of us had thought much about this, but within the last couple of weeks, he just had to find it. I wondered if he was looking for assurance that his heart was still functioning well after he had open heart surgery–a quadruple bypass and an aortic valve replacement in 2004. When we moved in 2014, I’m sure it was packed into a box and moved with us. However, we have searched everywhere in our small condo and it has not been found.
A couple of nights ago, he became quite distressed that the missing stethoscope had not been found, and became tearful. He had been sitting in his recliner resting for a while, so I did not immediately understand what caused his tears. Since I knew he had been “puttering” around the house in search for something, I asked: “What’s wrong? What are you looking for?” His response was “for my life.” Then it hit me. His old life, the one where he could hike, go kayaking, go camping, canoeing, and fishing, was lost. He was searching for it. I guess he was looking for his heart. It wasn’t really about the stethoscope.
I do not share his concern that his physical heart may not be in good shape, but I do fear that Parkinson’s has sapped his spirit. Depression is a common problem for people with Parkinson’s. Therefore, it is arguably more important to deal with depressive symptoms than it is to treat the physical mobility issues. If the body is willing but the spirit is weak, trouble ensues. George’s psychologist is just as important to his health as his neurologist.
Recently, I have been thinking a lot about the issue of “control.” What does it mean to be “in control,” and what does it mean to be “out of control?” Is control desirable? Do caregivers have control? Frankly, no one can control any other person, nor the progression of any disease. Neither the person with the disease, nor the caregivers, nor physicians and therapists, can control the outcome.
Do medications control anything? The answer to that is “yes,” to a degree. In our experience with Parkinson’s, only the symptoms are “controlled.” The root cause of the illness is not yet clearly understood, and there is no known cure. This is a frustrating thing, as our society has come to expect physicians to be “miracle workers” who can take care of any malady. It ain’t so!
Likewise, while our Creator may have numbered our days and counted each of the hairs on our heads, we are not able to control our longevity. Oh sure, we can exercise, eat properly, and watch all the chemicals we ingest into our bodies, but then we could be hit by a truck on the Interstate.
Lack of control in one area sometimes causes us to desire more control in another. If I cannot control the progression of George’s illness, then at least I can wash the dishes, clean house, keep the bills paid, and think about others’ needs. Those are all welcome distractions, actually. But, the desire for control can create problems with other relationships.
I think this was underscored to me the other night when our condo association met to discuss some important proposed community improvements. It was clear that everyone in the meeting had their own ideas about how to proceed with the project. No one person could (or should) control the outcome; rather, collaboration, negotiation, and compromise will ensure the best solution.
Joy and contentment are achieved by living in the moment, and not trying to control the behavior or thoughts of others. The words of The Serenity Prayer summarize this idea beautifully:
Serenity Prayer
God grant me the serenity
to accept the things I cannot change;
courage to change the things I can;
and wisdom to know the difference.
Living one day at a time;
Enjoying one moment at a time;
Accepting hardships as the pathway to peace;
Taking, as He did, this sinful world
as it is, not as I would have it;
Trusting that He will make all things right
if I surrender to His Will;
That I may be reasonably happy in this life
and supremely happy with Him
Forever in the next.
Amen.
Sounds simple, right? Certainly not! It is a constant effort to discern those things we can change and those things we cannot. For Parkinson’s Caregivers, The Serenity Prayer can help us find joy and contentment in the midst of day-to-day challenges.
If you’ve been in the caregiver game long enough, you know that in order to win the game, you must take care of yourself. For me, this includes attending musical events whenever possible.
Thanks to the kindness of season ticket holders, and the availability of George’s caregiver Greg, I was able to attend the final concert of the Knoxville Symphony Orchestra’s 2017-2018 season. It was a special joy because my dear friend Heather was able to attend the concert with me. The program was conducted by KSO Music Director Aram Demirjian, and highlighted by an excellent young pianist, Michelle Cann.
Aram Demirjian, KSO Music Director
An All-American program, it featured music composed by Bernstein, Florence Beatrice Price, George Gershwin, and Aaron Copland.
The concert began with a stirring rendition of Leonard Bernstein’s Overture to Candide (1956). According to the program notes, the American author Lillian Hellman suggested to Leonard Bernstein (perhaps as early as 1950) that the two of them collaborate on a musical adaptation of Voltaire’s Candide (1759). It took a few years, but the work has energy, lyricism, humor, and incredible emotional impact. The brief and rollicking overture has become a popular staple of concerts during the second half of the 20th century. It has a sparkling orchestration with many woodwinds, brass and percussion in addition to strings.
Michelle Cann, Pianist
Florence Beatrice Price was an African American composer born in Little Rock Arkansas in 1887. Her music was new to me, but I was happy to make its acquaintance. Her Concerto in One Movement for Piano and Orchestra (1934) contains three sections: Moderato – Adagio – Allegretto. It was extremely challenging writing for the soloist, but Michelle Cann’s assertive, bravura playing was up to the task. The concerto was notable for including traditional classical and folk elements. I especially noted the style of Scott Joplin’s Ragtime piano, and the finale thrilled us with the Juba, an African-American antebellum dance. It was so gratifying to see and hear such a talented African-American woman play the music of another African-American woman from a bygone age. Maestro Demirjian noted in his opening remarks that had she been male, Florence Beatrice Price’s name would be as well known as Gershwin or Joplin.
Gershwin’s Rhapsody in Blue (a personal favorite) completed the first half of the program. I have heard it many times played by several different pianists, and have multiple recordings of it as well. The opening clarinet “riff” is what we all await with unbridled anticipation and we love to hear. Unfortunately, Gary Sperl’s clarinet was not the best part; rather, Michelle Cann’s piano was every bit as virtuosic and emotionally charged as if George Gershwin himself had been on stage! The quintessential American concert jazz piece, The Rhapsody in Blue never fails to disappoint, but I doubt if I’ve ever enjoyed it more than on Friday evening, May 18.
If you love brass and percussion, you would have loved Aaron Copland’s Symphony No. 3 (1946). A rather lengthy piece, it is in four movements: Molto moderato, Allegro molto, Andantino quasi allegretto, and Allegro risoluto. In the words of Copland:
“I do borrow from myself by using Fanfare for the Common Man (1942) in an extended and reshaped form in the final movement. I used this opportunity to carry my Fanfare material further and to satisfy my desire to give the Third Symphony an affirmative tone. After all, it was a wartime piece–or more accurately, and end-of-war piece–intended to reflect the euphoric spirit of the country at the time.”
I cannot stress how much performing or listening to music does for my soul. For you as a caregiver, you may find reading, art, needlework, or other activities spiritually uplifting. Make sure as you manage medications, exercise, and diet for your loved one, you make time each day for yourself to rejuvenate, replenish, and recreate! We are all busy, but even 15 minutes a day devoted to a favorite activity can help you cope with stress. Both you and your loved one will be glad you did!
For people with Parkinson’s, assistive devices are a must. If you don’t need one today, there may be a day when you will. The progression of the disease differs from person to person, but it is likely that anyone diagnosed with Parkinson’s will require some kind of assistive device(s). And, different days present different challenges, so different kinds of devices are needed depending upon the stage of the illness and the amount of exercise the person does.
Walking is complicated business. Have you ever watched a toddler walk? He/she struggles with balance and putting one foot in front of the other. Walking for people with Parkinson’s is like that. It can be frustrating for the person afflicted as well as his/her caregiver(s). Once we learn how to walk, most of us tend to take it for granted unless we suffer from an accident or debilitating illness like Parkinson’s.
The first assistive device that George used was a traditional metal cane. this helped him for quite a while. Four years ago, it was all he needed for support.
Traditional Metal Canes
It was adjustable in length, but supported him on only one side. However, it was also relatively inexpensive, so it was a good first choice.
As his tremors were more pronounced on his right side (a phenomenon of Parkinson’s tremors seems to be that the dominant side is worse), he began to use the cane in his left hand, thereby putting more stress on the muscles of that side.
I believe that using a cane in one hand (his left) for a long time contributed to what recently has been diagnosed as a mild carpal tunnel syndrome.
The second cane we acquired was called the “Hurrycane.” This one was more stable because it features three feet at the bottom. Just like a three-legged stool, it is much harder to tip over. Another great thing about it was that it conveniently folded for travel. It could easily be stashed in a carryon bag to take up little space when travelling by air. I thought it was a clever, innovative design, but for an unknown reason, George seemed to prefer using the traditional metal can for quite a while.
The “Hurrycane”
As George’s mobility lessened, it became apparent that he needed to use a walker to provide a way for him to hold on with both hands while keeping him balanced. We purchased a walker manufactured by Drive. It features a flip up/flip down seat, is lightweight, and folds easily for travel.
Drive Medical Clever-Lite Walker
Primarily due to freezing episodes, George’s Occupational Therapist recommended an improved walker: the UStep II. Traditional rollators are difficult to move except in straight lines. The UStep II has a much better turning radius, and is more stable because of extra wheels. A laser light visual cue, and metronome-like audible cue provides guidance for where the user’s feet should be. Fortunately, we were able to have Medicare pay for this device, except for the optional storage bag and laser light.
UStep IIMedline Transport Chair
In January, 2017, George had to have some minor surgery unrelated to his Parkinson’s. We anticipated that he would be weaker after the general anesthesia. We decided that help would be needed to get home and get in and out of the car. So, we purchased a transport chair. It was day surgery, but thankfully, we were able to request the doctor to keep him overnight for observation. Even so, it was a good thing we had the chair. He was able to get into the car at the hospital, and get out of the car when we arrived home. However, he had a fall when he tried to move from the transport chair to his recliner.
Ever since, we have used it for long doctor visits where we need to make his transport easier. It is much lighter than a regular wheelchair, and I can easily fold and lift it to carry in the back of our small SUV. It is also lighter than the U Step II Walker. The good news is that most days we do not need this right now (he is in Stage 2 Parkinson’s), and the walker is all he needs.
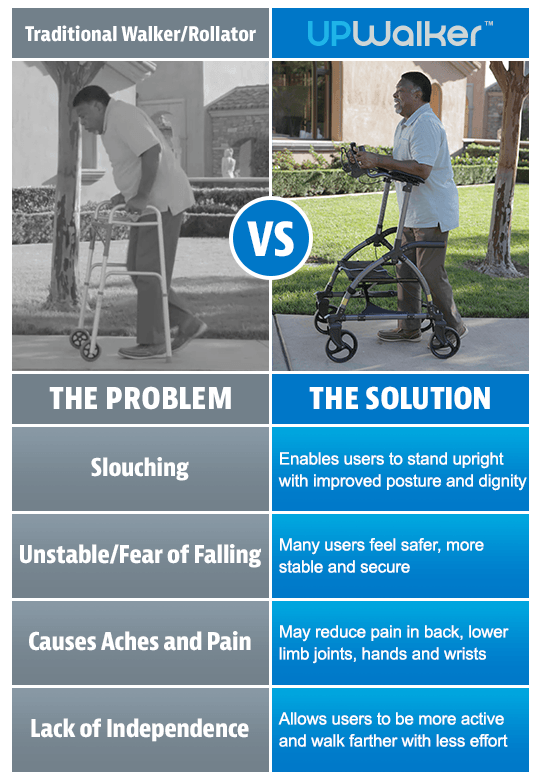
Recently, George acquired a new device! It encourages a more upright posture. The photos illustrate how a traditional walker/rollator can actually cause the user to have a more hunched-over posture. George has severe arthritis in his shoulder, and mild carpal tunnel syndrome in his wrist. This was exacerbated by weakness in his legs; he started pushing himself up and lowering himself down with his arms rather than using the glutes and leg muscles that are intended for such movements. He will require a physical therapist to teach him how to properly use this new device, as it works differently from the walkers he used previously. We are hopeful that this will help his posture, help to strengthen his back muscles, and improve his confidence. Mechanical assistive devices are great, but they should always be used with the assistance provided by caregivers, physical and/or occupational therapists. Fatigue and balance problems plague People with Parkinson’s, and the canes, walkers, or chairs should always be inspected frequently to ensure that the brakes work properly and that all parts are securely attached together.
Take care when using a new device, and make sure that your loved one understands how to safely use it. Consult a physical therapist if needed.
May 10 was Ascension Thursday. For those of you who may not share my faith tradition, Ascension is a big deal. The Feast of the Ascension of Jesus Christ, also known as Holy Thursday, Ascension Day, or Ascension Thursday, commemorates the Christian belief of the bodily Ascension of Jesus into heaven. It is one of the ecumenical feasts of Christian churches, ranking with the feasts of the Passion, of Easter, and Pentecost. Ascension Day is traditionally celebrated on a Thursday, the fortieth day of Easter, although some Christian denominations have moved the observance to the following Sunday.
The Episcopal Church of the Ascension in Knoxville celebrated Ascension Day in conjunction with Evening Prayer on May 10. I participated in that service as a Schola member. Our Schola prepares Gregorian chants and Psalms, which were prominent in Thursday evening’s service.
It was a busy evening! This followed the regular busyness of caring for George, which was particularly tiring on Wednesday of this past week. Neither one of us slept well on Wednesday night, so I was running on fumes.
As George’s primary “pill Nazi” I am obliged to remind him (when I’m home) that it is “pill time.” Having a smart phone helps with this, as I can set alarms for the six doses each day. It is very important that people with Parkinson’s take their medications at the prescribed times, otherwise “freezing” episodes (where they cannot move) ensue.
Frequently, our friend and caregiver Greg is with him when I sing at church, and that was the case Thursday night. Intellectually, at those times I know I do not need to have my phone with me (or powered on), but somehow I find it difficult to separate myself from what has become another appendage. I guess it provides some sort of emotional comfort, but why that is, I cannot tell because hearing those alarms actually adds to my stress.
Well, just as you can imagine, I did have my phone with me in the choir loft Thursday night. As we were chanting Psalm 96, (look it up if you are not familiar with the whole thing…) about the time we were chanting: “Worship the Lord in the beauty of holiness…” you guess it: the alarm went off! Had my ring tone been in the same key as the chant, it might not have been so bad, but it is always off-putting for musicians (especially singers) if random, stray pitches are heard. Andrew, our Schola Leader, said in a stage whisper: “Could someone cut that off??!!” Afterwards, Sister Kathleen asked Andrew what the unusual music was!
So, my alarm ascended to the rafters and to the heavens at the very moment that we were to sing to the Lord and bless his Name.
It has been said that no one dies of embarrassment, and that’s a good thing! Otherwise, I would be a goner. I don’t know about Andrew or Sister, but I am confident that our God of forgiveness forgave the recalcitrant smart phone.
There was a time when George was a “Type A” personality. His training as an accountant required him to be precise, and a stickler for details. He cared a lot about many things: me, our children, his work, and his happy avocation as Boy Scout Leader. That was then.
Now we face apathetic days. More troubling than his physical symptoms is his lack of interest in activities he once enjoyed. The dictionary defines apathy as follows:
A study documented in the Journal of Neurology, Neurosurgery and Psychiatry concluded:
Apathy in Parkinson’s disease is more likely to be a direct consequence of disease related physiological changes than a psychological reaction or adaptation to disability. Apathy in Parkinson’s disease can be distinguished from other psychiatric symptoms and personality features that are associated with the disease, and it is closely associated with cognitive impairment. These findings point to a possible role of cognitive mechanisms in the expression of apathy.
Given that conclusion, we have been striving to address George’s mobility challenges. His physician has added Clonazepam (a medication to induce REM sleep) and Rasagiline (a medication to even out the “on” and “off” periods of his Carbidopa-Levodopa doses). The new pharmaceutical cocktail seems to be working.
Thus far, we are seeing a gradual improvement in his sleep quality and his ease of mobility. A milestone for us was this morning when he (unprompted by me) walked to the newspaper box to bring in the paper! We are hopeful that things will continue to improve.
At the same time, I and George’s regular caregiver are encouraging him to get out of the house more and interact with family members. It is an uphill battle, but we continue the fight. We don’t want to return to the “Type A Days” but “Type B” wouldn’t be too bad!







 Mechanical assistive devices are great, but they should always be used with the assistance provided by caregivers, physical and/or occupational therapists. Fatigue and balance problems plague People with Parkinson’s, and the canes, walkers, or chairs should always be inspected frequently to ensure that the brakes work properly and that all parts are securely attached together.
Mechanical assistive devices are great, but they should always be used with the assistance provided by caregivers, physical and/or occupational therapists. Fatigue and balance problems plague People with Parkinson’s, and the canes, walkers, or chairs should always be inspected frequently to ensure that the brakes work properly and that all parts are securely attached together.